Ketogenic: The Science of Therapeutic Carbohydrate Restriction in Human Health presents the most up-to-date and evidence-based science and research available in the field of TCR, with the purpose of training medical and allied healthcare professionals on the effective therapeutic use of low-carbohydrate and ketogenic nutrition in clinical practice. This book explores the appropriate, safe, and effective use of TCR to improve patient outcomes in a broad range of chronic metabolic conditions and aims to promote health.
Focused on lifestyle management, health support and the treatment of diseases rooted in poor nutrition, this book explores the role of food and lifestyle modification as medicine and is a valuable resource for nutritionists, dietitians and medical professionals who provide diet-related counselling, as well as those researching or studying related areas.
- Presents new best-practice guidelines for using TCR to treat, improve or reverse nutrition-related metabolic conditions and diseases that were previously thought to have a chronic, irreversible progression
- Provides an overview of the most recent evidence outlining the biochemistry and physiology pertaining to human nutrition and health
- Offers evolutionary and historical context to human nutrition
- Contains clinical practice guidelines for the implementation of TCR from medical practitioners who prescribe TCR in their practices, allowing readers to understand real-life concerns in the field
- Features case studies that provide practical examples of how to assess, monitor and intervene with patients that practitioners encounter in their practices
- Explains the physiology and biochemistry of the normal and pathophysiological state for each condition and links these to the application of TCR
https://doi.org/10.1016/C2019-0-03604-7 Full Book is available on the normal book sharing websites.
Chapter 1 - Understanding human diet, disease, and insulin resistance: scientific and evolutionary perspectives
Nutritional authorities promote high-carbohydrate, low-fat diets to combat modern diseases such as obesity, type 2 diabetes and heart disease. However, the science behind this ideology is flawed. Virtually everything the public knows about diet can be challenged. The foods that cause harm are the very food groups the public believes are healthy: carbohydrates and polyunsaturated vegetable oils. Conversely, human physiology, from brain size to gastrointestinal morphology appears to support a carnivorous design. While low amounts of certain carbohydrates are tolerable, chronic consumption of processed carbohydrates promotes non-communicable diseases (NCDs). Indigenous cultures adopting modern agriculture develop diseases practically absent beforehand. Processed foods have been linked to systemic inflammation, mitochondrial dysfunction, and more. Their mechanism is insulin resistance, which is crucially involved in most NCDs. The chronic disease pandemic only worsens despite the billions of dollars invested to treat them. A new perspective is needed.
Chapter 2 - Nutritional aspects
With evidence pointing to the efficacy of therapeutic carbohydrate restriction (TCR), official protocols for implementation into clinical practice are required. During the metabolic transition from a high-carbohydrate to a TCR diet, clinical considerations and patient guidance are required. Aside from the formulation and prescription of TCR, clinicians must be familiar with the precautions, assessment, and monitoring of clinical outcomes associated with this intervention. Nutritional ketosis is a physiological ketosis of the fed state with specific biochemical and nutritional aspects that must be taken into account in TCR. Understanding this metabolic state, as well as the biochemistry and physiology of ketone metabolism, is critical. When prescribing TCR, the clinician must also understand the context of nutrient requirements, as well as the differences between animal and plant nutrition. This chapter discusses the most important nutritional aspects to consider and comprehend when prescribing TCR.
Chapter 3 - Endocrine
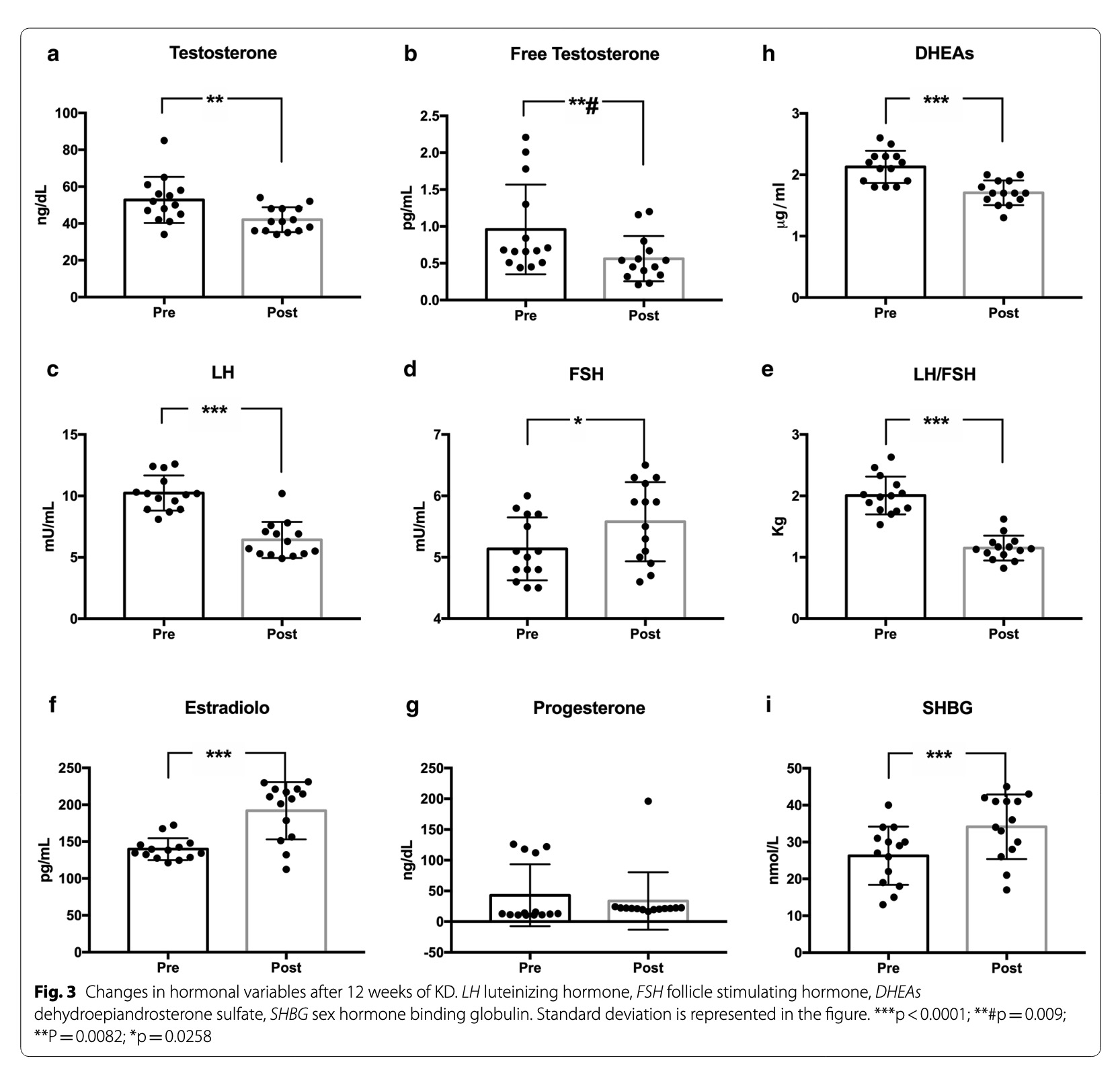
Endocrine dysregulation is the hallmark of modern chronic disease, with insulin resistance (IR) playing a central role. Research surrounding treatments to such disorders are complicated due to complex hormonal regulation of homoeostasis, with the liver playing a central role. Yet recognising the common pathology provides a more universally applicable approach to treatment: the target and regulation of insulin. Therapeutic carbohydrate restriction (TCR) has efficacy in regulating insulin, often without the need for, or with the deprescription of, pharmacotherapeutics. The most evidence for TCR focuses on its induced remission of metabolic syndrome (MetS), IR, and type 2 diabetes (T2D). Emerging research also supports its use for type 1 diabetes (T1D), polycystic ovarian syndrome (PCOS) and regulation of the thyroid and the hypothalamic-pituitary-adrenal-axis. Overall, TCR is promising in the treatment of endocrine disorders, often surpassing many medications prescribed to treat them.
Chapter 4 - Cardiovascular disease and its association with insulin resistance and cholesterol
As the main nutrient delivery system, the cardiovascular system is intimately tied to metabolic health. Insulin resistance (IR) is implicated in atherosclerosis through numerous pathophysiologies, causing a variety of problems from stroke and renal failure to congestive heart failure (CHF) and myocardial infarction (MI). The traditional atherosclerosis model, the diet (lipid) heart hypothesis, wrongly demonises LDL, a biologically essential, multifunctional transport molecule, which is more likely atheroprotective than atherogenic. The resultant prescription of cholesterol-lowering medications (statins and PCSK9 inhibitors) arguably worsen heart health and IR. Evidence is presented for the role of therapeutic carbohydrate restriction (TCR), despite its high fat and cholesterol content, in reducing IR and improving overall cardiometabolic risk (lipids and blood pressure).
Chapter 5 - Neurology
The brain is a metabolically demanding organ and thus sensitive to nutrient availability. It is not ordinarily conceived to be predisposed to metabolic syndromes, though research postulates insulin resistance and chronic hyperglycaemia may be behind most neurological disorders, redefining them from a metabolic perspective. High-carbohydrate diets also have an important psychological impact. The brain has been evolutionarily programmed to treat carbohydrates as a reward, activating dopaminergic cascades due to their historical scarcity. This neurobiology has disadvantages in an age of carbohydrate abundance. While the brain is perceived as a glucose-dependent organ, ketone bodies are an alternative and possibly superior fuel, allowing patients with Alzheimer’s disease (AD), dementia, and mood disorders to improve their glucose hypometabolic states and associated symptoms. Ketogenic diets (KDs) are an accepted standard of treatment for refractory epilepsies and alleviate neuroinflammation in other neuropathologies. Research on the KD in the treatment of these disorders is in its infancy, yet has demonstrable restorative potential begging further investigation.
Chapter 6 - Cancer
Since the discovery of DNA, the metabolic theory of cancer has been sidelined for genetic research. Yet cancer continues to rise. New research recaptures mitochondria as the driver, while upregulation of oncogenes and tumour suppressor mutations are recognised as downstream of the damage to oxidative phosphorylation (OxPhos). Despite the prevalence of the somatic (genetic) mutation theory, there are numerous inconsistencies. In contrast, it appears that all cancers are characterised by dysfunctional mitochondria. Cancer pre-1960 was a rare disease, all of which has changed as diets have. Press-pulse therapy and ketogenic diets (KD) have proven effective therapies, due to cancers’ selective metabolism of glucose and glutamine (Warburg effect), in combination with the non-fermentability of ketones. Some dietary aspects are individualised to the patient and cancer, but follow this general protocol. Fasting induces additional selective stress to cancers. With cancer genetic research stagnating and metabolic approaches showing promise, this perspective offers a new path forward.
Chapter 7 - Musculoskeletal and immunological considerations
Musculoskeletal conditions are primarily thought to be age-related and unavoidable. While age is a factor for musculoskeletal functional decline, an association with age should be considered alongside lifestyle factors. Inflammation accompanies musculoskeletal conditions, and should be targeted when considering interventions for these conditions. Diet is a key modulator of inflammation. The Western diet is known to contribute to inflammation and can negatively affect the microbiome, both of which are implicated in autoimmune disease. Therapeutic carbohydrate restriction (TCR), on the other hand, shows promise for improving inflammation and the microbiome, as well as rheumatic and autoimmune conditions. As it relates to age-associated declines, a well-formulated TCR protocol naturally is animal nutrient-centric, meaning it supplies sufficient protein, minerals, and fat-soluble vitamins to prevent or delay chronic conditions and bone and joint issues, supplemented with exercise (which itself demonstrates similar preventative effects). TCR, in addition to metabolic improvement, has well-documented effects of improvement in age associated physiology, such as visceral adiposity, decline of cognition, bone mass, density, and muscle mass, and increased risk for chronic disease associated mortality. In this chapter the role of TCR as a promising supportive treatment for many rheumatic and autoimmune conditions, as well as age-related conditions is discussed.
Chapter 8 - Gastrointestinal health and therapeutic carbohydrate restriction
Human health is tied to the microbiome, and dysbiosis begets disease. Many gastrointestinal (GI) conditions cause unnecessary proliferation of normal gut microbiota, leading to dysbiosis, painful symptoms and hunger signal dysregulation. Dysbiosis causes damage to tight junctions and provides an entryway for pathogens to systemic circulation, which leads to a variety of conditions, including allergies, intolerances and even autoimmune reactions. Other disorders exist in the liver, pancreas, hepatic portal system and gallbladder, all of which follow from poor dietary choices. Therapeutic carbohydrate restriction or the ketogenic diet (KD) is, by nature, closely related to diets with evidence of efficacy for various GI conditions (namely, specific carbohydrate diet and low-FODMAP diets). Unsurprisingly then, evidence is emerging regarding a similar efficacy. The KD is animal-based and as such excludes many plant-based gut irritants. Some troubleshooting and individualisation may be required, but an adapted KD has long-term clinical potential to alleviate many GI conditions and deserves more clinical application.
Chapter 9 - Exercise and sports performance
The role of fat adaptation and carbohydrate restriction for athletes is an emerging and controversial area. Many athletes voice concern over glycogen depletion with carbohydrate-restricted diets. Though, with mounting metabolic concerns of chronic excessive carbohydrate consumption manifesting in athletes, alternative ergogenic protocols need be devised to sustain health and performance in athletes. Much research on the metabolic effects of ketogenic diets (KDs) and low carbohydrate, high fat (LCHF) diets and related supplementation in athletes is ongoing. Most literature concentrates on high-carbohydrate male athletes and cannot apply to ketogenic or female athletes without considering metabolic differences. The research that has surfaced on KDs maligns it with performance impairment due to trial brevity. Other studies accounting for the extensive period of metabolic reprogramming generally show performance maintenance or improvement. Athletic nutrition and performance are individualised and troubleshooting may be needed. Case studies have emerged of KDs showing benefit in some athletes, emphasising the need for clinical trials.
Chapter 10 - Therapeutic fasting
Fasting is a voluntary, controlled period of abstinence from food that is important to human evolution and has medical, spiritual, and cultural significance in most areas of the world. However, in Westernised countries, incidence and duration of fasting has decreased due to dietary emphasis on snacking. This shift has profound health effects due to the continual suppression of fasting-state gluconeogenesis, nutritional ketosis, and protein conservation, often resetting the cycle before blood glucose and insulin falls. Patients may voice concerns over malnutrition or nutrient depletion, though evidence underscores the physiological differences between fasting (benefits) and starvation (complications). Contraindications and cautions are few but require consideration. Fasting is an effective regimen as it minimises time and financial expenditure, in addition to having health benefits and enhancing longevity.
Chapter 11 - Psychological, behavioural, and ethical considerations
A dietary intervention is only effective in the long term if it is sustainable. Sustainable health improvements require persistent changes in thoughts and behaviour, as well as control over eating. There are techniques healthcare practitioners can employ to guide patients towards behaviour change, while encouraging them to take responsibility for their own health and achieve lasting improvements. Therapeutic carbohydrate restriction (TCR), gives patients a physiological advantage by controlling hunger (despite reduced caloric intake and weight loss); offering a sustainable alternative to conventional hypocaloric weight loss interventions, which usually result in hunger and rebound weight gains. Evidence indicates that ultra-processed food (UPF) may also play a role in cravings and eating control, promoting addictive eating behaviours that thwart health and weight loss efforts. TCR eliminates UPF and thus, as an adjunct to other behavioural and psychological interventions, may offer a treatment modality to address addictive eating. While TCR is a relatively novel nutritional evidence-based modality that challenges current dietary guidelines, healthcare practitioners have an ethical responsibility to fulfil the Hippocratic values that underlie western medical ethics, to first do no harm. In the light of evidence indicating the harmful effects of conventional high-carbohydrate diets on metabolic health, TCR public health advocacy is one of the most crucial ethical duties of healthcare professionals in modern times.