TLDR: The current advice that LDL is "bad cholesterol", appears to be outdated, and the actual situation is more complex. In people over 60 high LDL appeared to be protective for mortality.
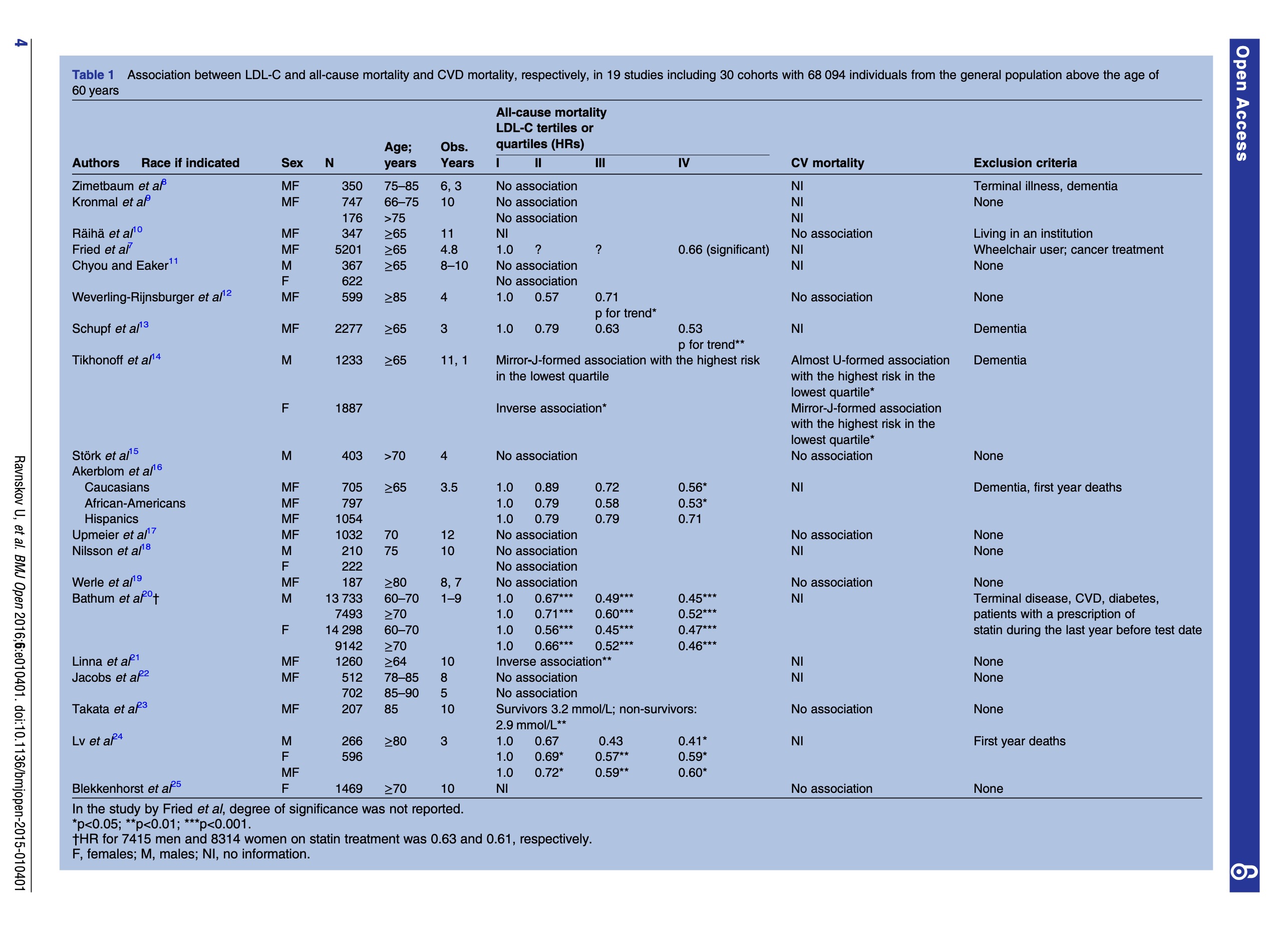
Conclusions: High LDL-C is inversely associated with mortality in most people over 60 years. This finding is inconsistent with the cholesterol hypothesis (ie, that cholesterol, particularly LDL-C, is inherently atherogenic). Since elderly people with high LDL-C live as long or longer than those with low LDL-C, our analysis provides reason to question the validity of the cholesterol hypothesis. Moreover, our study provides the rationale for a re-evaluation of guidelines recommending pharmacological reduction of LDL-C in the elderly as a component of cardiovascular disease prevention strategies.
Full Paper at https://pubmed.ncbi.nlm.nih.gov/27292972/
Related to, and following up on the LMHR paper from https://hackertalks.com/post/5835924
.